The Treatment And Cause Of Over-Pronation Of The Foot
Overview
Pronation is a normal motion that our feet make as they walk. With each step, the heel touches the ground first, then the foot rolls forward to the toes, causing the ankle to roll inward slightly and the arch to flatten out. That?s normal. But when that rolling inward becomes more pronounced, that?s over-pronation, which is a big problem. You can usually see over-pronation by looking at the back of the leg and foot. The Achilles tendon normally runs straight down from the leg to the foot, hitting the floor at a perpendicular angle. In feet that over-pronate, the Achilles tendon will be at a slight angle to the ground and the ankle bone will appear more prominent than usual.
Causes
Unless there is a severe, acute injury, overpronation develops as a gradual biomechanical distortion. Several factors contribute to developing overpronation, including tibialis posterior weakness, ligament weakness, excess weight, pes planus (flat foot), genu valgum (knock knees), subtalar eversion, or other biomechanical distortions in the foot or ankle. Tibialis posterior weakness is one of the primary factors leading to overpronation. Pronation primarily is controlled by the architecture of the foot and eccentric activation of the tibialis posterior. If the tibialis posterior is weak, the muscle cannot adequately slow the natural pronation cycle.
Symptoms
Due to the laxity of the soft tissue structures of the foot, and the fact that the joints are not held together properly, the bones of the feet shift. When this occurs, the muscles that attach to these bones must also shift, or twist, in order to attach to these bones. The strongest and most important muscles that attach to our foot bones come from our lower leg. So, as these muscles course down the leg and across the ankle, they must twist to maintain their proper attachments in the foot. This twisting of these muscles will cause shin splints, Achilles Tendonitis, generalized tendonitis, fatigue, muscle aches and pains, cramps, ankle sprains, and loss of muscular efficiency (reducing walking and running speed and endurance). The problems we see in the feet, which are due to over-pronation include bunions, heel spurs, plantar fasciitis, fallen and painful arches, hammertoes, metatarsalgia (ball of foot pain), and calluses.
Diagnosis
The best way to discover whether you have a normal gait, or if you overpronate, is to visit a specialty run shop, an exercise physiologist, a podiatrist or a physical therapist who specializes in working with athletes. A professional can analyze your gait, by watching you either walk or run, preferably on a treadmill. Some facilities can videotape your gait, then analyze the movement of your feet in slow-motion. Another (and less costly) way is to look at the bottom of an older pair of run shoes. Check the wear pattern. A person with a normal gait will generally see wear evenly across the heel and front of the shoe. A person who overpronates will likely see more wear on the OUTside of the heel and more wear on the INside of the forefoot (at the ball). A person who supinates will see wear all along the outer edges of the shoe. You can also learn about your gait by looking at your arches. Look at the shape your wet feet leave on a piece of paper or a flat walking surface.
Non Surgical Treatment
Studies have shown that the most effective way to dexrease a high Q angle and lower the biomechanical stresses on the knee joint is to prevent excessive pronation with custom-maflexible orthotics. One study found that using soft corrective orthotics was more effective in reduknee pain than a traditional exercise program. A more recent study showed that Q angle asymmetries, secondary to excessive pronation affecting knee alignment, can be effectivecontrolled or corrected utilizing custom-made, flexible orthotics. Another project involving meof a running club determined that 75% of those using orthotics eliminated or greatly reduced pain in the feet, ankles, shins, knees and hips
Prevention
Massage and stretch the calves to increase dorsiflexion at the foot/ankle. Dorsiflexion is the bending at the ankle. By improving the dorsiflexion, one will have more flexibility at the ankle, which will allow the foot to over-pronate less. Massage the IT Band with a foam roller or tennis ball to quiet down the tightness throughout this part of the leg. The IT Band attaches from the glute maximus and runs down the side of the leg into the knee area. When the IT Band is tight it will accelerate the force of the leg moving inward, which will cause the foot to move inward as well. It is often that tightness through the IT Band that promotes over-pronation. Decreasing over-pronation, which is very prominent in runners, will help add endurance, speed and efficiency to your run and ultimately place less stress on your body.
Pronation is a normal motion that our feet make as they walk. With each step, the heel touches the ground first, then the foot rolls forward to the toes, causing the ankle to roll inward slightly and the arch to flatten out. That?s normal. But when that rolling inward becomes more pronounced, that?s over-pronation, which is a big problem. You can usually see over-pronation by looking at the back of the leg and foot. The Achilles tendon normally runs straight down from the leg to the foot, hitting the floor at a perpendicular angle. In feet that over-pronate, the Achilles tendon will be at a slight angle to the ground and the ankle bone will appear more prominent than usual.
Causes
Unless there is a severe, acute injury, overpronation develops as a gradual biomechanical distortion. Several factors contribute to developing overpronation, including tibialis posterior weakness, ligament weakness, excess weight, pes planus (flat foot), genu valgum (knock knees), subtalar eversion, or other biomechanical distortions in the foot or ankle. Tibialis posterior weakness is one of the primary factors leading to overpronation. Pronation primarily is controlled by the architecture of the foot and eccentric activation of the tibialis posterior. If the tibialis posterior is weak, the muscle cannot adequately slow the natural pronation cycle.
Symptoms
Due to the laxity of the soft tissue structures of the foot, and the fact that the joints are not held together properly, the bones of the feet shift. When this occurs, the muscles that attach to these bones must also shift, or twist, in order to attach to these bones. The strongest and most important muscles that attach to our foot bones come from our lower leg. So, as these muscles course down the leg and across the ankle, they must twist to maintain their proper attachments in the foot. This twisting of these muscles will cause shin splints, Achilles Tendonitis, generalized tendonitis, fatigue, muscle aches and pains, cramps, ankle sprains, and loss of muscular efficiency (reducing walking and running speed and endurance). The problems we see in the feet, which are due to over-pronation include bunions, heel spurs, plantar fasciitis, fallen and painful arches, hammertoes, metatarsalgia (ball of foot pain), and calluses.
Diagnosis
The best way to discover whether you have a normal gait, or if you overpronate, is to visit a specialty run shop, an exercise physiologist, a podiatrist or a physical therapist who specializes in working with athletes. A professional can analyze your gait, by watching you either walk or run, preferably on a treadmill. Some facilities can videotape your gait, then analyze the movement of your feet in slow-motion. Another (and less costly) way is to look at the bottom of an older pair of run shoes. Check the wear pattern. A person with a normal gait will generally see wear evenly across the heel and front of the shoe. A person who overpronates will likely see more wear on the OUTside of the heel and more wear on the INside of the forefoot (at the ball). A person who supinates will see wear all along the outer edges of the shoe. You can also learn about your gait by looking at your arches. Look at the shape your wet feet leave on a piece of paper or a flat walking surface.
Non Surgical Treatment
Studies have shown that the most effective way to dexrease a high Q angle and lower the biomechanical stresses on the knee joint is to prevent excessive pronation with custom-maflexible orthotics. One study found that using soft corrective orthotics was more effective in reduknee pain than a traditional exercise program. A more recent study showed that Q angle asymmetries, secondary to excessive pronation affecting knee alignment, can be effectivecontrolled or corrected utilizing custom-made, flexible orthotics. Another project involving meof a running club determined that 75% of those using orthotics eliminated or greatly reduced pain in the feet, ankles, shins, knees and hips
Prevention
Massage and stretch the calves to increase dorsiflexion at the foot/ankle. Dorsiflexion is the bending at the ankle. By improving the dorsiflexion, one will have more flexibility at the ankle, which will allow the foot to over-pronate less. Massage the IT Band with a foam roller or tennis ball to quiet down the tightness throughout this part of the leg. The IT Band attaches from the glute maximus and runs down the side of the leg into the knee area. When the IT Band is tight it will accelerate the force of the leg moving inward, which will cause the foot to move inward as well. It is often that tightness through the IT Band that promotes over-pronation. Decreasing over-pronation, which is very prominent in runners, will help add endurance, speed and efficiency to your run and ultimately place less stress on your body.
Severs Disease Physiotherapy
Overview
Sever's Disease, also known as calcaneal apophysitis, is a disease of the growth plate of the bone and is characterized by pain in the heel of a child's foot, typically brought on by some form of injury or trauma. This condition is most common in children ages 10 to 15 and is frequently seen in active soccer, football, or baseball players. Sport shoes with cleats are also known to aggravate the condition. The disease mimics Achilles tendonitis, an inflammation of the tendon attached to the back of the heel. A tight Achilles tendon contributes to Sever's Disease by pulling excessively on the growth plate of the heel bone (calcaneus). Treatment includes cutting back on sports activities, calf muscle stretching exercises, heel cushions in the shoes, icing, and/or anti-inflammatory medications. Note: Please consult your physician before taking any medications.
Causes
Apart from age, other factors that may contribute to developing Sever?s disease include physical activity, any form of exercise that is weight bearing through the legs or stresses the soft tissue can exacerbate the pain of the disease, External factors, for example, running on hard surfaces or wearing inappropriate shoes during sport Overuse injury, very active children may repeatedly but subtly injure the bones, muscles and tendons of their feet and ankles. In time, the accumulated injuries cause symptoms.
Symptoms
The most common symptom of Sever's disease is acute pain felt in the heel when a child engages in physical activity such as walking, jumping or running. Children who are very active athletes are among the group most susceptible to experiencing Sever's disease because of the extreme stress and tension they place on their growing feet. Improper pronation, the rolling movement of the foot during walking or running, and obesity are all additional conditions linked to causing Sever's disease.
Diagnosis
A doctor can usually tell that a child has Sever's disease based on the symptoms reported. To confirm the diagnosis, the doctor will probably examine the heels and ask about the child's activity level and participation in sports. The doctor might also use the squeeze test, squeezing the back part of the heel from both sides at the same time to see if doing so causes pain. The doctor might also ask the child to stand on tiptoes to see if that position causes pain. Although imaging tests such as X-rays generally are not that helpful in diagnosing Sever's disease, some doctors order them to rule out other problems, such as fractures. Sever's disease cannot be seen on an X-ray.
Non Surgical Treatment
Most patients with Sever?s Disease can be treated with a self-guided home exercise program. Your healthcare provider will discuss with you if a prescription for formal physical therapy is indicated instead of a self-directed home or school exercise program. Rest (protection of the heel). Ice (Ice 20 minutes at a time, 2-3 times a day). Gel heel pads / inserts. Anti-inflammatory medication. Well cushioned pair of shoes. Brace (Cheetah) *Generally given for those who cannot wear shoes during their sport. Low impact aerobic training such as walking, riding a bike, elliptical or swimming. Home exercise program focusing on increasing the flexibility of the heel cord and calf muscle.
Recovery
Severs disease is a self limiting condition that gradually resolves as the patient moves towards skeletal maturity. This usually takes between 6 to 12 months, but may persist for as long as 2 years. With appropriate management, symptoms may resolve in a number of weeks. Patients with Severs disease typically improve gradually over time and full function is restored.
Sever's Disease, also known as calcaneal apophysitis, is a disease of the growth plate of the bone and is characterized by pain in the heel of a child's foot, typically brought on by some form of injury or trauma. This condition is most common in children ages 10 to 15 and is frequently seen in active soccer, football, or baseball players. Sport shoes with cleats are also known to aggravate the condition. The disease mimics Achilles tendonitis, an inflammation of the tendon attached to the back of the heel. A tight Achilles tendon contributes to Sever's Disease by pulling excessively on the growth plate of the heel bone (calcaneus). Treatment includes cutting back on sports activities, calf muscle stretching exercises, heel cushions in the shoes, icing, and/or anti-inflammatory medications. Note: Please consult your physician before taking any medications.
Causes
Apart from age, other factors that may contribute to developing Sever?s disease include physical activity, any form of exercise that is weight bearing through the legs or stresses the soft tissue can exacerbate the pain of the disease, External factors, for example, running on hard surfaces or wearing inappropriate shoes during sport Overuse injury, very active children may repeatedly but subtly injure the bones, muscles and tendons of their feet and ankles. In time, the accumulated injuries cause symptoms.
Symptoms
The most common symptom of Sever's disease is acute pain felt in the heel when a child engages in physical activity such as walking, jumping or running. Children who are very active athletes are among the group most susceptible to experiencing Sever's disease because of the extreme stress and tension they place on their growing feet. Improper pronation, the rolling movement of the foot during walking or running, and obesity are all additional conditions linked to causing Sever's disease.
Diagnosis
A doctor can usually tell that a child has Sever's disease based on the symptoms reported. To confirm the diagnosis, the doctor will probably examine the heels and ask about the child's activity level and participation in sports. The doctor might also use the squeeze test, squeezing the back part of the heel from both sides at the same time to see if doing so causes pain. The doctor might also ask the child to stand on tiptoes to see if that position causes pain. Although imaging tests such as X-rays generally are not that helpful in diagnosing Sever's disease, some doctors order them to rule out other problems, such as fractures. Sever's disease cannot be seen on an X-ray.
Non Surgical Treatment
Most patients with Sever?s Disease can be treated with a self-guided home exercise program. Your healthcare provider will discuss with you if a prescription for formal physical therapy is indicated instead of a self-directed home or school exercise program. Rest (protection of the heel). Ice (Ice 20 minutes at a time, 2-3 times a day). Gel heel pads / inserts. Anti-inflammatory medication. Well cushioned pair of shoes. Brace (Cheetah) *Generally given for those who cannot wear shoes during their sport. Low impact aerobic training such as walking, riding a bike, elliptical or swimming. Home exercise program focusing on increasing the flexibility of the heel cord and calf muscle.
Recovery
Severs disease is a self limiting condition that gradually resolves as the patient moves towards skeletal maturity. This usually takes between 6 to 12 months, but may persist for as long as 2 years. With appropriate management, symptoms may resolve in a number of weeks. Patients with Severs disease typically improve gradually over time and full function is restored.
The Causes Of Posterior Tibial Tendon Dysfunction (PTTD) ?
Overview
Adult Acquired Flatfoot (Posterior Tibial Tendon Dysfunction) is a painful, progressive deformity in adults. It results from a gradual stretch (attenuation) of the tibialis posterior tendon and the ligaments that support your foot?s arch. This stretching causes the tendon to lose strength and function. Many people have flat feet and do not experience pain. However, pain occurs with Adult Acquired Flatfoot because the tendons and ligaments have been torn. Once the vital ligaments and posterior tibial tendon are lost, there is no longer anything holding the arch of the foot in place. 
Causes
Women are affected by Adult Acquired Flatfoot four times more frequently than men. Adult Flatfoot generally occurs in middle to older age people. Most people who acquire the condition already have flat feet. One arch begins to flatten more, then pain and swelling develop on the inside of the ankle. This condition generally affects only one foot. It is unclear why women are affected more often than men. But factors that may increase your risk of Adult Flatfoot include diabetes, hypertension, and obesity.
Symptoms
Depending on the cause of the flatfoot, a patient may experience one or more of the different symptoms here. Pain along the course of the posterior tibial tendon which lies on the inside of the foot and ankle. This can be associated with swelling on the inside of the ankle. Pain that is worse with activity. High intensity or impact activities, such as running, can be very difficult. Some patients can have difficulty walking or even standing for long periods of time. When the foot collapses, the heel bone may shift position and put pressure on the outside ankle bone (fibula). This can cause pain on the outside of the ankle. Arthritis in the heel also causes this same type of pain. Patients with an old injury or arthritis in the middle of the foot can have painful, bony bumps on the top and inside of the foot. These make shoewear very difficult. Occasionally, the bony spurs are so large that they pinch the nerves which can result in numbness and tingling on the top of the foot and into the toes. Diabetics may only notice swelling or a large bump on the bottom of the foot. Because their sensation is affected, people with diabetes may not have any pain. The large bump can cause skin problems and an ulcer (a sore that does not heal) may develop if proper diabetic shoewear is not used.
Diagnosis
Posterior Tibial Tendon Dysfunction is diagnosed with careful clinical observation of the patient?s gait (walking), range of motion testing for the foot and ankle joints, and diagnostic imaging. People with flatfoot deformity walk with the heel angled outward, also called over-pronation. Although it is normal for the arch to impact the ground for shock absorption, people with PTTD have an arch that fully collapses to the ground and does not reform an arch during the entire gait period. After evaluating the ambulation pattern, the foot and ankle range of motion should be tested. Usually the affected foot will have decreased motion to the ankle joint and the hindfoot. Muscle strength may also be weaker as well. An easy test to perform for PTTD is the single heel raise where the patient is asked to raise up on the ball of his or her effected foot. A normal foot type can lift up on the toes without pain and the heel will invert slightly once the person has fully raised the heel up during the test. In early phases of PTTD the patient may be able to lift up the heel but the heel will not invert. An elongated or torn posterior tibial tendon, which is a mid to late finding of PTTD, will prohibit the patient from fully rising up on the heel and will cause intense pain to the arch. Finally diagnostic imaging, although used alone cannot diagnose PTTD, can provide additional information for an accurate diagnosis of flatfoot deformity. Xrays of the foot can show the practitioner important angular relationships of the hindfoot and forefoot which help diagnose flatfoot deformity. Most of the time, an MRI is not needed to diagnose PTTD but is a tool that should be considered in advanced cases of flatfoot deformity. If a partial tear of the posterior tibial tendon is of concern, then an MRI can show the anatomic location of the tear and the extensiveness of the injury.
Non surgical Treatment
Nonoperative therapy for adult-acquired flatfoot is a reasonable treatment option that is likely to be beneficial for most patients. In this article, we describe the results of a retrospective cohort study that focused on nonoperative measures, including bracing, physical therapy, and anti-inflammatory medications, used to treat adult-acquired flatfoot in 64 consecutive patients. The results revealed the incidence of successful nonsurgical treatment to be 87.5% (56 of 64 patients), over the 27-month observation period. Overall, 78.12% of the patients with adult-acquired flatfoot were obese (body mass index [BMI] = 30), and 62.5% of the patients who failed nonsurgical therapy were obese; however, logistic regression failed to show that BMI was statistically significantly associated with the outcome of treatment. The use of any form of bracing was statistically significantly associated with successful nonsurgical treatment (fully adjusted OR = 19.8621, 95% CI 1.8774 to 210.134), whereas the presence of a split-tear of the tibialis posterior on magnetic resonance image scans was statistically significantly associated with failed nonsurgical treatment (fully adjusted OR = 0.016, 95% CI 0.0011 to 0.2347). The results of this investigation indicate that a systematic nonsurgical treatment approach to the treatment of the adult-acquired flatfoot deformity can be successful in most cases. 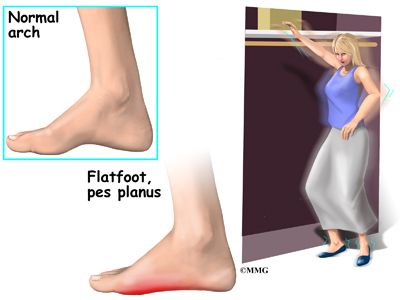
Surgical Treatment
Stage two deformities are less responsive to conservative therapies that can be effective in mild deformities. Bone procedures are necessary at this stage in order to recreate the arch and stabilize the foot. These procedures include isolated fusion procedures, bone grafts, and/or the repositioning of bones through cuts called osteotomies. The realigned bones are generally held in place with screws, pins, plates, or staples while the bone heals. A tendon transfer may or may not be utilized depending on the condition of the posterior tibial tendon. Stage three deformities are better treated with surgical correction, in healthy patients. Patients that are unable to tolerate surgery or the prolonged healing period are better served with either arch supports known as orthotics or bracing such as the Richie Brace. Surgical correction at this stage usually requires fusion procedures such as a triple or double arthrodesis. This involves fusing the two or three major bones in the back of the foot together with screws or pins. The most common joints fused together are the subtalar joint, talonavicular joint, and the calcaneocuboid joint. By fusing the bones together the surgeon is able to correct structural deformity and alleviate arthritic pain. Tendon transfer procedures are usually not beneficial at this stage. Stage four deformities are treated similarly but with the addition of fusing the ankle joint.
Pain In The Arch Causes Symptoms And Treatments
Overview
One of those often-painful soft tissue that attaches to heel spurs at the bottom of the foot is called "plantar fascia". Fascia, located throughout the body, is a fibrous connective tissue similar to a ligament. You can see fascia when you handle meat. It is the white, connective tissue separating layers of meat or attaching to bones. The "plantar" fascia in our bodies is that fascia which is seen on the bottom (or plantar portion) of the foot, extending from the heel bone to the ball of the foot. Compared to other fascia around the body, plantar fascia is very thick and very strong. It has to be strong because of the tremendous amount of force it must endure when you walk, run or jump. But while the plantar fascia is a strong structure, it can still get injured, most commonly when it is stretched beyond its normal length over long periods of time. When plantar fascia is injured, the condition is called "plantar fasciitis", which is usualy pronounced either "plan-tar fash-I-tis" or "plan-tar-fash-ee-I-tis." (Adding "-itis" to the end of a word means that structure is inflamed.) It is sometimes known more simply as 'fasciitis'. Plantar fasciitis is the most common type of arch pain.

Causes
The plantar fascia is designed to absorb the high stresses and strains we place on our feet. But, sometimes, too much pressure damages or tears the tissues. The body's natural response to injury is inflammation, which results in the heel pain and stiffness of plantar fasciitis.
Symptoms
The primary symptom is pain or aching in the arch area. This can be accompanied by inflammation and tenderness. If the pain is caused by the plantar fascia, it is likely to be considerably more severe in the mornings due to the muscles being unused.
Diagnosis
Your doctor may order imaging tests to help make sure your heel pain is caused by plantar fasciitis and not another problem. X-rays provide clear images of bones. They are useful in ruling out other causes of heel pain, such as fractures or arthritis. Heel spurs can be seen on an x-ray. Other imaging tests, such as magnetic resonance imaging (MRI) and ultrasound, are not routinely used to diagnose plantar fasciitis. They are rarely ordered. An MRI scan may be used if the heel pain is not relieved by initial treatment methods.
Non Surgical Treatment
Treatment for a high arch foot or Charcot Marie Tooth disorder depends on the extent of deformity and the amount of disability experienced by the patient. Depending upon the symptoms, treatment may include. Changing the shoes. Special orthotic supports (devices that support, adjust, or accommodate the foot deformity). Cushioning pads. Foot and ankle braces or surgery.

Surgical Treatment
In cases where cast immobilization, orthoses and shoe therapy have failed, surgery is the next alternative. The goal of surgery and non-surgical treatment is to eliminate pain, stop progression of the deformity and improve mobility of the patient. Opinions vary as to the best surgical treatment for adult acquired flatfoot. Procedures commonly used to correct the condition include tendon debridement, tendon transfers, osteotomies (cutting and repositioning of bone) and joint fusions.
Prevention
To prevent arch pain, it is important to build up slowly to your exercise routine while wearing arch supports inside training shoes. By undertaking these simple measures you can prevent the discomfort of arch pain which can otherwise linger for many months. While you allow the foot to recover, it will help to undertake low impact exercises (such as swimming or water aerobics).
Stretching Exercises
Inchworm. Stand with your weight on one foot. Raise the metatarsal heads of the unweighted foot while you pull its heel closer to your toes. Next, raise your toes toward the ceiling, and then relax your whole foot with it flat on the floor. Your foot should move like an inchworm across the floor. Reps 6-7 for each foot. Horsepawing. Stand with your weight on one foot and the other foot slightly in front of you. Raise the metatarsal heads on the front foot. Lift your heel ever so slightly off the ground, maintaining the raised metatarsal heads, and pull your foot toward you so that it ends up behind you. Return this foot to the starting position in front of you. You should really feel this one in your arch. Reps. 6-7 for each foot. Toe pushups. Sit in a chair with your feet resting on the floor. Raise your heel as high as you can while keeping your toes flat on the floor. This is the starting position. Using your toe muscles, roll your foot upward until the weight of your foot is resting on the ends of your toes, like a dancer standing on point in toe shoes. Roll back down to the starting position. Reps. 10-20 for each foot. Sand scraping. Pretend you are at the beach standing in loose sand. Use your big toe to pull sand inward toward your body, with your little toe off the ground. Then use your little toe to push it away, with your big toe off the ground. Reps. 10 for each foot. Now reverse the exercise: pull the sand inward with your little toe and push it away with your big toe. Reps. 10 for each foot.
One of those often-painful soft tissue that attaches to heel spurs at the bottom of the foot is called "plantar fascia". Fascia, located throughout the body, is a fibrous connective tissue similar to a ligament. You can see fascia when you handle meat. It is the white, connective tissue separating layers of meat or attaching to bones. The "plantar" fascia in our bodies is that fascia which is seen on the bottom (or plantar portion) of the foot, extending from the heel bone to the ball of the foot. Compared to other fascia around the body, plantar fascia is very thick and very strong. It has to be strong because of the tremendous amount of force it must endure when you walk, run or jump. But while the plantar fascia is a strong structure, it can still get injured, most commonly when it is stretched beyond its normal length over long periods of time. When plantar fascia is injured, the condition is called "plantar fasciitis", which is usualy pronounced either "plan-tar fash-I-tis" or "plan-tar-fash-ee-I-tis." (Adding "-itis" to the end of a word means that structure is inflamed.) It is sometimes known more simply as 'fasciitis'. Plantar fasciitis is the most common type of arch pain.
Causes
The plantar fascia is designed to absorb the high stresses and strains we place on our feet. But, sometimes, too much pressure damages or tears the tissues. The body's natural response to injury is inflammation, which results in the heel pain and stiffness of plantar fasciitis.
Symptoms
The primary symptom is pain or aching in the arch area. This can be accompanied by inflammation and tenderness. If the pain is caused by the plantar fascia, it is likely to be considerably more severe in the mornings due to the muscles being unused.
Diagnosis
Your doctor may order imaging tests to help make sure your heel pain is caused by plantar fasciitis and not another problem. X-rays provide clear images of bones. They are useful in ruling out other causes of heel pain, such as fractures or arthritis. Heel spurs can be seen on an x-ray. Other imaging tests, such as magnetic resonance imaging (MRI) and ultrasound, are not routinely used to diagnose plantar fasciitis. They are rarely ordered. An MRI scan may be used if the heel pain is not relieved by initial treatment methods.
Non Surgical Treatment
Treatment for a high arch foot or Charcot Marie Tooth disorder depends on the extent of deformity and the amount of disability experienced by the patient. Depending upon the symptoms, treatment may include. Changing the shoes. Special orthotic supports (devices that support, adjust, or accommodate the foot deformity). Cushioning pads. Foot and ankle braces or surgery.
Surgical Treatment
In cases where cast immobilization, orthoses and shoe therapy have failed, surgery is the next alternative. The goal of surgery and non-surgical treatment is to eliminate pain, stop progression of the deformity and improve mobility of the patient. Opinions vary as to the best surgical treatment for adult acquired flatfoot. Procedures commonly used to correct the condition include tendon debridement, tendon transfers, osteotomies (cutting and repositioning of bone) and joint fusions.
Prevention
To prevent arch pain, it is important to build up slowly to your exercise routine while wearing arch supports inside training shoes. By undertaking these simple measures you can prevent the discomfort of arch pain which can otherwise linger for many months. While you allow the foot to recover, it will help to undertake low impact exercises (such as swimming or water aerobics).
Stretching Exercises
Inchworm. Stand with your weight on one foot. Raise the metatarsal heads of the unweighted foot while you pull its heel closer to your toes. Next, raise your toes toward the ceiling, and then relax your whole foot with it flat on the floor. Your foot should move like an inchworm across the floor. Reps 6-7 for each foot. Horsepawing. Stand with your weight on one foot and the other foot slightly in front of you. Raise the metatarsal heads on the front foot. Lift your heel ever so slightly off the ground, maintaining the raised metatarsal heads, and pull your foot toward you so that it ends up behind you. Return this foot to the starting position in front of you. You should really feel this one in your arch. Reps. 6-7 for each foot. Toe pushups. Sit in a chair with your feet resting on the floor. Raise your heel as high as you can while keeping your toes flat on the floor. This is the starting position. Using your toe muscles, roll your foot upward until the weight of your foot is resting on the ends of your toes, like a dancer standing on point in toe shoes. Roll back down to the starting position. Reps. 10-20 for each foot. Sand scraping. Pretend you are at the beach standing in loose sand. Use your big toe to pull sand inward toward your body, with your little toe off the ground. Then use your little toe to push it away, with your big toe off the ground. Reps. 10 for each foot. Now reverse the exercise: pull the sand inward with your little toe and push it away with your big toe. Reps. 10 for each foot.
What Are The Symptoms Of An Achilles Tendon Rupture
Overview  The Achilles tendon connects the muscles in the back of your calf to your heel bone. There are two basic variations of Achilles injuries. Achilles tendonitis, and a complete tear. It?s important to know whether the Achilles is torn or not, because the treatment is very different, a torn Achilles may require surgery. Achilles tendonitis probably means rehab and rest. While tendonitis is a gradual onset of pain that tends to get worse with more activity, an Achilles tear is a sudden injury, and it feels as if you were hit or kicked in the back of the ankle. A tear usually affects your ability to walk properly. Because an Achilles tendon rupture can impair your ability to walk, it?s common to seek immediate treatment. You may also need to consult with doctors specializing in sports medicine or orthopaedic surgery. Causes The Achilles tendon is most commonly injured by sudden plantarflexion or dorsiflexion of the ankle, or by forced dorsiflexion of the ankle outside its normal range of motion. Other mechanisms by which the Achilles can be torn involve sudden direct trauma to the tendon, or sudden activation of the Achilles after atrophy from prolonged periods of inactivity. Some other common tears can occur from overuse while participating in intense sports. Twisting or jerking motions can also contribute to injury. Fluoroquinolone antibiotics, famously ciprofloxacin, are known to increase the risk of tendon rupture, particularly achilles. Symptoms Ankle pain and swelling or feeling like the ankle has ?given out? after falling or stumbling. A loud audible pop when the ankle is injured. Patients may have a history of prior ankle pain or Achilles tendonitis, and may be active in sports. Swelling, tenderness and possible discoloration or ecchymosis in the Achilles tendon region. Indentation above the injured tendon where the torn tendon may be present. Difficulty moving around or walking. Individual has difficulty or is unable to move their ankle with full range of motion. MRI can confirm disruption or tear in the tendon. Inability to lift the toes. Diagnosis Diagnosis is made by clinical history; typically people say it feels like being kicked or shot behind the ankle. Upon examination a gap may be felt just above the heel unless swelling has filled the gap and the Simmonds' test (aka Thompson test) will be positive; squeezing the calf muscles of the affected side while the patient lies prone, face down, with his feet hanging loose results in no movement (no passive plantarflexion) of the foot, while movement is expected with an intact Achilles tendon and should be observable upon manipulation of the uninvolved calf. Walking will usually be severely impaired, as the patient will be unable to step off the ground using the injured leg. The patient will also be unable to stand up on the toes of that leg, and pointing the foot downward (plantarflexion) will be impaired. Pain may be severe, and swelling is common. Sometimes an ultrasound scan may be required to clarify or confirm the diagnosis. MRI can also be used to confirm the diagnosis. Non Surgical Treatment Non-surgical treatment of Achilles tendon rupture is usually reserved for patients who are relatively sedentary or may be at higher risk for complications with surgical intervention (due to other associated medical problems). This involves a period of immobilization, followed by range of motion and strengthening exercises; unfortunately, it is associated with a higher risk of re-rupture of the tendon, and possibly a less optimal functional outcome.
The Achilles tendon connects the muscles in the back of your calf to your heel bone. There are two basic variations of Achilles injuries. Achilles tendonitis, and a complete tear. It?s important to know whether the Achilles is torn or not, because the treatment is very different, a torn Achilles may require surgery. Achilles tendonitis probably means rehab and rest. While tendonitis is a gradual onset of pain that tends to get worse with more activity, an Achilles tear is a sudden injury, and it feels as if you were hit or kicked in the back of the ankle. A tear usually affects your ability to walk properly. Because an Achilles tendon rupture can impair your ability to walk, it?s common to seek immediate treatment. You may also need to consult with doctors specializing in sports medicine or orthopaedic surgery. Causes The Achilles tendon is most commonly injured by sudden plantarflexion or dorsiflexion of the ankle, or by forced dorsiflexion of the ankle outside its normal range of motion. Other mechanisms by which the Achilles can be torn involve sudden direct trauma to the tendon, or sudden activation of the Achilles after atrophy from prolonged periods of inactivity. Some other common tears can occur from overuse while participating in intense sports. Twisting or jerking motions can also contribute to injury. Fluoroquinolone antibiotics, famously ciprofloxacin, are known to increase the risk of tendon rupture, particularly achilles. Symptoms Ankle pain and swelling or feeling like the ankle has ?given out? after falling or stumbling. A loud audible pop when the ankle is injured. Patients may have a history of prior ankle pain or Achilles tendonitis, and may be active in sports. Swelling, tenderness and possible discoloration or ecchymosis in the Achilles tendon region. Indentation above the injured tendon where the torn tendon may be present. Difficulty moving around or walking. Individual has difficulty or is unable to move their ankle with full range of motion. MRI can confirm disruption or tear in the tendon. Inability to lift the toes. Diagnosis Diagnosis is made by clinical history; typically people say it feels like being kicked or shot behind the ankle. Upon examination a gap may be felt just above the heel unless swelling has filled the gap and the Simmonds' test (aka Thompson test) will be positive; squeezing the calf muscles of the affected side while the patient lies prone, face down, with his feet hanging loose results in no movement (no passive plantarflexion) of the foot, while movement is expected with an intact Achilles tendon and should be observable upon manipulation of the uninvolved calf. Walking will usually be severely impaired, as the patient will be unable to step off the ground using the injured leg. The patient will also be unable to stand up on the toes of that leg, and pointing the foot downward (plantarflexion) will be impaired. Pain may be severe, and swelling is common. Sometimes an ultrasound scan may be required to clarify or confirm the diagnosis. MRI can also be used to confirm the diagnosis. Non Surgical Treatment Non-surgical treatment of Achilles tendon rupture is usually reserved for patients who are relatively sedentary or may be at higher risk for complications with surgical intervention (due to other associated medical problems). This involves a period of immobilization, followed by range of motion and strengthening exercises; unfortunately, it is associated with a higher risk of re-rupture of the tendon, and possibly a less optimal functional outcome.  Surgical Treatment There are two different types of surgeries; open surgery and percutaneous surgery. During an open surgery an incision is made in the back of the leg and the Achilles tendon is stitched together. In a complete or serious rupture the tendon of plantaris or another vestigial muscle is harvested and wrapped around the Achilles tendon, increasing the strength of the repaired tendon. If the tissue quality is poor, e.g. the injury has been neglected, the surgeon might use a reinforcement mesh (collagen, Artelon or other degradable material). In percutaneous surgery, the surgeon makes several small incisions, rather than one large incision, and sews the tendon back together through the incision(s). Surgery may be delayed for about a week after the rupture to let the swelling go down. For sedentary patients and those who have vasculopathy or risks for poor healing, percutaneous surgical repair may be a better treatment choice than open surgical repair.
Surgical Treatment There are two different types of surgeries; open surgery and percutaneous surgery. During an open surgery an incision is made in the back of the leg and the Achilles tendon is stitched together. In a complete or serious rupture the tendon of plantaris or another vestigial muscle is harvested and wrapped around the Achilles tendon, increasing the strength of the repaired tendon. If the tissue quality is poor, e.g. the injury has been neglected, the surgeon might use a reinforcement mesh (collagen, Artelon or other degradable material). In percutaneous surgery, the surgeon makes several small incisions, rather than one large incision, and sews the tendon back together through the incision(s). Surgery may be delayed for about a week after the rupture to let the swelling go down. For sedentary patients and those who have vasculopathy or risks for poor healing, percutaneous surgical repair may be a better treatment choice than open surgical repair.
Pes Planus Causes And Symptoms
Overview
Flexible flatfeet are considered normal in young children because babies are not born with a normal arch. The arch may not form fully until sometime between ages 7 and 10. Even in adulthood, 15% to 25% of people have flexible flatfeet. Most of these people never develop symptoms. In many adults who have had flexible flatfeet since childhood, the missing arch is an inherited condition related to a general looseness of ligaments. These people usually have extremely flexible, very mobile joints throughout the body, not only in the feet. Flatfeet also can develop during adulthood. Causes include joint disease, such as rheumatoid arthritis, and disorders of nerve function (neuropathy). Unlike a flexible flatfoot, a rigid flatfoot is often the result of a significant problem affecting the structure or alignment of the bones that make up the foot's arch. Some common causes of rigid flatfeet include. Congenital vertical talus. In this condition, there is no arch because the foot bones are not aligned properly. In some cases, there is a reverse curve (rocker-bottom foot, in which the shape is like the bottom rails of a rocking chair) in place of the normal arch. Congenital vertical talus is a rare condition present at birth. It often is associated with a genetic disorder, such as Down syndrome, or other congenital disorders. The cause is unknown in up to half of cases. Tarsal coalition (peroneal spastic flatfoot). In this inherited condition, two or more of the foot bones are fused together, interfering with the flexibility of the foot and eliminating the normal arch. A rare condition, it often affects several generations of the same family. Lateral subtalar dislocation. Sometimes called an acquired flatfoot, it occurs in someone who originally had a normal foot arch. In a lateral subtalar dislocation, there is a dislocation of the talus bone, located within the arch of the foot. The dislocated talus bone slips out of place, drops downward and sideways and collapses the arch. It usually occurs suddenly because of a high-impact injury related to a fall from a height, a motor vehicle accident or participation in sports, and it may be associated with fractures or other injuries.
Causes
The most common acquired flat foot in adults is due to Posterior Tibial Tendon Dysfunction. This develops with repetitive stress on the main supporting tendon of the arch over a long period of time. As the body ages, ligaments and muscles can weaken, leaving the job of supporting the arch all to this tendon. The tendon cannot hold all the weight for long, and it gradually gives out, leading to a progressively lower arch. This form of flat foot is often accompanied by pain radiating behind the ankle, consistent with the course of the posterior tibial tendon. Compounding matters is the fact that the human foot was not originally designed to withstand the types of terrain and forces it is subjected to today. Nowhere in nature do you see the flat hard surfaces that we so commonly walk on in present times. Walking on this type of surface continuously puts unnatural stress on the arch. The fact that the average American is overweight does not help the arch much either-obesity is a leading cause of flat feet as the arch collapses under the excessive bodyweight. Furthermore, the average life span has increased dramatically in the last century, meaning that not only does the arch deal with heavy weight on hard flat ground, but also must now do so for longer periods of time. These are all reasons to take extra care of our feet now in order to prevent problems later.
Symptoms
Flat feet may not cause any symptoms at all. Rigid flat feet may cause pain, calluses, blisters, or skin redness on the inner side of the foot. A stiff foot, weakness or numbness of the foot, Rapid wearing out of shoes-worn shoes lean in toward each other. Difficulty or pain with activities like running-in the foot, knee or hip.
Diagnosis
If your child has flatfeet, his or her doctor will ask about any family history of flatfeet or inherited foot problems. In a person of any age, the doctor will ask about occupational and recreational activities, previous foot trauma or foot surgery and the type of shoes worn. The doctor will examine your shoes to check for signs of excessive wear. Worn shoes often provide valuable clues to gait problems and poor bone alignment. The doctor will ask you to walk barefoot to evaluate the arches of the feet, to check for out-toeing and to look for other signs of poor foot mechanics. The doctor will examine your feet for foot flexibility and range of motion and feel for any tenderness or bony abnormalities. Depending on the results of this physical examination, foot X-rays may be recommended. X-rays are always performed in a young child with rigid flatfeet and in an adult with acquired flatfeet due to trauma.
Non Surgical Treatment
The treatment your podiatrist recommends will depend upon the trouble and pain you?re experiencing. Custom shoe inserts (orthotics) are most often recommended and are quite effective. Stretching exercises to loosen and strengthen the supporting tendons may also be recommended. Orthotic devices or bracing. To give your arch the support it needs, your foot and ankle surgeon may recommend an ankle brace or a custom orthotic device that fits into your shoe to support the arch. A short-leg cast or boot may be worn to immobilize the foot and allow the tendon to heal. Ultrasound therapy and stretching exercises may help rehabilitate the tendon and muscle following immobilization. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Your foot and ankle surgeon may recommend changes in your footwear.
Surgical Treatment

Since there are many different causes of flatfoot, the types of flatfoot reconstruction surgery are best categorized by the conditions. Posterior tibial tendon dysfunction. In this condition, the tendon connecting the calf muscle to the inner foot is torn or inflamed. Once the tendon is damaged it no longer can serve its main function of supporting the arch of the foot. Flatfoot is the main result of this type of condition and can be treated by the following flatfoot reconstruction surgeries. Lengthening of the Achilles tendon. Otherwise known as gastrocnemius recession, this procedure is used to lengthen the calf muscles in the leg. This surgery treats flatfoot and prevents it from returning in the future. This procedure is often combined with other surgeries to correct posterior tibial tendon dysfunction. Cleaning the tendon. Also known as tenosynovectomy, this procedure is used in the earlier and less severe stages of posterior tibial tendon dysfunction. It is performed before the arch collapses and while the tendon is only mildly affected. The inflamed tissue is cleaned away and removed from the remaining healthy tendon. Tendon transfer. This procedure is done to correct flatfoot and reform the lost arch in the foot. During the procedure, the diseased tendon is removed and replaced by tendon from another area of the foot. If the tendon is only partially damaged, the inflamed part is cleaned and removed then attached to a new tendon. Cutting and shifting bones. Also called an osteotomy, this procedure consists of cutting and reconstructing bones in the foot to reconstruct the arch. The heel bone and the midfoot are most likely reshaped to achieve this desired result. A bone graft may be used to fuse the bones or to lengthen the outside of the foot. Temporary instrumentation such as screws and plates can also be used to hold the bones together while they heal.
Prevention
Sit up straight in a chair with your feet flat on the ground. Scrunch up the toes of one foot as if you are trying to grab hold of the floor then use your toes to drag your foot a small distance forwards. Do this a couple of times on each foot, but don?t use your leg muscles to push your foot forward -- the movement should come solely from the muscles in your feet. Sit in a chair and place a cleaning cloth, towel or small ball on the floor at your feet. Use the toes of one foot to grasp the object and lift it off the floor. This action will require you to clench your toes and contract your arch. Once you have lifted the object a little way off the floor, try to throw it in the air and catch it by stretching your toes and arch out and upwards. Repeat the exercise several times on both feet. Sit on the floor with your legs straight out in front of you then bend your knees out to either side and place the soles of your feet together so your legs form a diamond. Hold on to your ankles and, keeping your heels together at all times, separate your feet so your toes point out to either side. Open and close your feet in this way several times, making sure your little toes stay in contact with the floor throughout the exercise. Starting in the same position, try separating your heels, keeping your toes together at all times.
After Care
Time off work depends on the type of work as well as the surgical procedures performed. . A patient will be required to be non-weight bearing in a cast or splint and use crutches for four to twelve weeks. Usually a patient can return to work in one to two weeks if they are able to work while seated. If a person's job requires standing and walking, return to work may take several weeks. Complete recovery may take six months to a full year. Complications can occur as with all surgeries, but are minimized by strictly following your surgeon's post-operative instructions. The main complications include infection, bone that is slow to heal or does not heal, progression or reoccurrence of deformity, a stiff foot, and the need for further surgery. Many of the above complications can be avoided by only putting weight on the operative foot when allowed by your surgeon.
Flexible flatfeet are considered normal in young children because babies are not born with a normal arch. The arch may not form fully until sometime between ages 7 and 10. Even in adulthood, 15% to 25% of people have flexible flatfeet. Most of these people never develop symptoms. In many adults who have had flexible flatfeet since childhood, the missing arch is an inherited condition related to a general looseness of ligaments. These people usually have extremely flexible, very mobile joints throughout the body, not only in the feet. Flatfeet also can develop during adulthood. Causes include joint disease, such as rheumatoid arthritis, and disorders of nerve function (neuropathy). Unlike a flexible flatfoot, a rigid flatfoot is often the result of a significant problem affecting the structure or alignment of the bones that make up the foot's arch. Some common causes of rigid flatfeet include. Congenital vertical talus. In this condition, there is no arch because the foot bones are not aligned properly. In some cases, there is a reverse curve (rocker-bottom foot, in which the shape is like the bottom rails of a rocking chair) in place of the normal arch. Congenital vertical talus is a rare condition present at birth. It often is associated with a genetic disorder, such as Down syndrome, or other congenital disorders. The cause is unknown in up to half of cases. Tarsal coalition (peroneal spastic flatfoot). In this inherited condition, two or more of the foot bones are fused together, interfering with the flexibility of the foot and eliminating the normal arch. A rare condition, it often affects several generations of the same family. Lateral subtalar dislocation. Sometimes called an acquired flatfoot, it occurs in someone who originally had a normal foot arch. In a lateral subtalar dislocation, there is a dislocation of the talus bone, located within the arch of the foot. The dislocated talus bone slips out of place, drops downward and sideways and collapses the arch. It usually occurs suddenly because of a high-impact injury related to a fall from a height, a motor vehicle accident or participation in sports, and it may be associated with fractures or other injuries.
Causes
The most common acquired flat foot in adults is due to Posterior Tibial Tendon Dysfunction. This develops with repetitive stress on the main supporting tendon of the arch over a long period of time. As the body ages, ligaments and muscles can weaken, leaving the job of supporting the arch all to this tendon. The tendon cannot hold all the weight for long, and it gradually gives out, leading to a progressively lower arch. This form of flat foot is often accompanied by pain radiating behind the ankle, consistent with the course of the posterior tibial tendon. Compounding matters is the fact that the human foot was not originally designed to withstand the types of terrain and forces it is subjected to today. Nowhere in nature do you see the flat hard surfaces that we so commonly walk on in present times. Walking on this type of surface continuously puts unnatural stress on the arch. The fact that the average American is overweight does not help the arch much either-obesity is a leading cause of flat feet as the arch collapses under the excessive bodyweight. Furthermore, the average life span has increased dramatically in the last century, meaning that not only does the arch deal with heavy weight on hard flat ground, but also must now do so for longer periods of time. These are all reasons to take extra care of our feet now in order to prevent problems later.
Symptoms
Flat feet may not cause any symptoms at all. Rigid flat feet may cause pain, calluses, blisters, or skin redness on the inner side of the foot. A stiff foot, weakness or numbness of the foot, Rapid wearing out of shoes-worn shoes lean in toward each other. Difficulty or pain with activities like running-in the foot, knee or hip.
Diagnosis
If your child has flatfeet, his or her doctor will ask about any family history of flatfeet or inherited foot problems. In a person of any age, the doctor will ask about occupational and recreational activities, previous foot trauma or foot surgery and the type of shoes worn. The doctor will examine your shoes to check for signs of excessive wear. Worn shoes often provide valuable clues to gait problems and poor bone alignment. The doctor will ask you to walk barefoot to evaluate the arches of the feet, to check for out-toeing and to look for other signs of poor foot mechanics. The doctor will examine your feet for foot flexibility and range of motion and feel for any tenderness or bony abnormalities. Depending on the results of this physical examination, foot X-rays may be recommended. X-rays are always performed in a young child with rigid flatfeet and in an adult with acquired flatfeet due to trauma.
Non Surgical Treatment
The treatment your podiatrist recommends will depend upon the trouble and pain you?re experiencing. Custom shoe inserts (orthotics) are most often recommended and are quite effective. Stretching exercises to loosen and strengthen the supporting tendons may also be recommended. Orthotic devices or bracing. To give your arch the support it needs, your foot and ankle surgeon may recommend an ankle brace or a custom orthotic device that fits into your shoe to support the arch. A short-leg cast or boot may be worn to immobilize the foot and allow the tendon to heal. Ultrasound therapy and stretching exercises may help rehabilitate the tendon and muscle following immobilization. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Your foot and ankle surgeon may recommend changes in your footwear.
Surgical Treatment
Since there are many different causes of flatfoot, the types of flatfoot reconstruction surgery are best categorized by the conditions. Posterior tibial tendon dysfunction. In this condition, the tendon connecting the calf muscle to the inner foot is torn or inflamed. Once the tendon is damaged it no longer can serve its main function of supporting the arch of the foot. Flatfoot is the main result of this type of condition and can be treated by the following flatfoot reconstruction surgeries. Lengthening of the Achilles tendon. Otherwise known as gastrocnemius recession, this procedure is used to lengthen the calf muscles in the leg. This surgery treats flatfoot and prevents it from returning in the future. This procedure is often combined with other surgeries to correct posterior tibial tendon dysfunction. Cleaning the tendon. Also known as tenosynovectomy, this procedure is used in the earlier and less severe stages of posterior tibial tendon dysfunction. It is performed before the arch collapses and while the tendon is only mildly affected. The inflamed tissue is cleaned away and removed from the remaining healthy tendon. Tendon transfer. This procedure is done to correct flatfoot and reform the lost arch in the foot. During the procedure, the diseased tendon is removed and replaced by tendon from another area of the foot. If the tendon is only partially damaged, the inflamed part is cleaned and removed then attached to a new tendon. Cutting and shifting bones. Also called an osteotomy, this procedure consists of cutting and reconstructing bones in the foot to reconstruct the arch. The heel bone and the midfoot are most likely reshaped to achieve this desired result. A bone graft may be used to fuse the bones or to lengthen the outside of the foot. Temporary instrumentation such as screws and plates can also be used to hold the bones together while they heal.
Prevention
Sit up straight in a chair with your feet flat on the ground. Scrunch up the toes of one foot as if you are trying to grab hold of the floor then use your toes to drag your foot a small distance forwards. Do this a couple of times on each foot, but don?t use your leg muscles to push your foot forward -- the movement should come solely from the muscles in your feet. Sit in a chair and place a cleaning cloth, towel or small ball on the floor at your feet. Use the toes of one foot to grasp the object and lift it off the floor. This action will require you to clench your toes and contract your arch. Once you have lifted the object a little way off the floor, try to throw it in the air and catch it by stretching your toes and arch out and upwards. Repeat the exercise several times on both feet. Sit on the floor with your legs straight out in front of you then bend your knees out to either side and place the soles of your feet together so your legs form a diamond. Hold on to your ankles and, keeping your heels together at all times, separate your feet so your toes point out to either side. Open and close your feet in this way several times, making sure your little toes stay in contact with the floor throughout the exercise. Starting in the same position, try separating your heels, keeping your toes together at all times.
After Care
Time off work depends on the type of work as well as the surgical procedures performed. . A patient will be required to be non-weight bearing in a cast or splint and use crutches for four to twelve weeks. Usually a patient can return to work in one to two weeks if they are able to work while seated. If a person's job requires standing and walking, return to work may take several weeks. Complete recovery may take six months to a full year. Complications can occur as with all surgeries, but are minimized by strictly following your surgeon's post-operative instructions. The main complications include infection, bone that is slow to heal or does not heal, progression or reoccurrence of deformity, a stiff foot, and the need for further surgery. Many of the above complications can be avoided by only putting weight on the operative foot when allowed by your surgeon.
Fallen Arches Causes And Symptoms
Overview

They make it possible for us to walk, run, and stand. With over two dozen bones, your feet are really a masterpiece of engineering. But sometimes even the best made things have flaws. One common problem is to have flatfeet, or fallen arches.
Causes
Abnormal development of the foot, producing Pes Planus, may be due to neurological problems, eg cerebral palsy, polio. Bony or ligamentous abnormalities, eg tarsal coalition (fusion of tarsal bones), accessory navicular bone. A small proportion of flexible flat feet do not correct with growth. Some of these may become rigid if the Pes Planus leads to bony changes.
Symptoms
Most patients who suffer from flat feet or fallen arches often do not complain of any symptoms whatsoever. However, on some occasions, patients may find that their feet are fatigued fairly easily and following activity on long periods of standing may have a painful foot or arch. On occasions, swelling may be seen on the inner aspect of the foot and performing certain movements may be painful and difficult. Some patients who have flat feet may find that their feet tend to roll in (over-pronate) a lot more when they walk and run. As a result, they may experience damage to the ankle joint and the Achilles tendon, as well as excessive shoe wear.
Diagnosis
If you notice that your feet are flat, but you?re not really experiencing any pain, then you?re probably okay to go without a visit to the podiatrist (unless, of course, you have a lack of feeling in your foot). You can schedule a hair appointment instead, or maybe see a movie. However, once painful symptoms start to appear, it?s better to skip the hirsute (or cinematic) experience and go see your foot doctor. Your podiatrist will likely make the diagnosis by examining your foot visually, asking about symptoms you may be experiencing, and may test your muscle strength. You may be asked to stand on your toes (in a ballerina pose, if you prefer, although that?s certainly not required), or walk around the examining room, and you may need to show the podiatrist your shoes. He or she may comment on your excellent taste in footwear, but is more likely to check your shoes for signs of wear that may indicate fallen arches. Your podiatrist may recommend X-rays, a CT scan or an MRI in order to get a look at the interior of your foot, although the best diagnosis usually comes from the doctor?s own in-person examination.
Non Surgical Treatment
Foot orthotic devices can stabilize some of the causes of flat feet, optimize muscle function and reduce the occurrence of painful symptoms. Generally, a custom-made semi-rigid functional posted orthotic is effective for flat feet. These devices are prescribed based on a thorough biomechanical examination by a qualified chiropodist/podiatrist. Over-the-counter arch supports may be helpful for mild cases, but often prove ineffective to relieve symptoms associated with flatfoot. Wear shoes with a good fit in the arch. Keep active and fit to strengthen leg and foot musculature. Control body weight to decrease load on the feet. Avoid prolonged periods weight bearing with bare feet. Taping to support strained ligaments and joints. Physical therapy modalities such as ultrasound. Referral for surgical correction a severe symptomatic flatfoot.
Surgical Treatment

Surgery for flat feet is separated into three kinds: soft tissue procedures, bone cuts, and bone fusions. Depending on the severity of the flat foot, a person?s age, and whether or not the foot is stiff determines just how the foot can be fixed. In most cases a combination of procedures are performed. With flexible flat feet, surgery is geared at maintaining the motion of the foot and recreating the arch. Commonly this may involve tendon repairs along the inside of the foot to reinforce the main tendon that lifts the arch. When the bone collapse is significant, bone procedures are included to physically rebuild the arch, and realign the heel. The presence of bunions with flat feet is often contributing to the collapse and in most situations requires correction. With rigid flat feet, surgery is focused on restoring the shape of the foot through procedures that eliminate motion. In this case, motion does not exist pre-operatively, so realigning the foot is of utmost importance. The exception, are rigid flat feet due to tarsal coalition (fused segment of bone) in the back of the foot where freeing the blockage can restore function.
Prevention
Going barefoot, particularly over terrain such as a beach where muscles are given a good workout, is good for all but the most extremely flatfooted, or those with certain related conditions such as plantar fasciitis. Ligament laxity is also among the factors known to be associated with flat feet. One medical study in India with a large sample size of children who had grown up wearing shoes and others going barefoot found that the longitudinal arches of the bare footers were generally strongest and highest as a group, and that flat feet were less common in children who had grown up wearing sandals or slippers than among those who had worn closed-toe shoes. Focusing on the influence of footwear on the prevalence of pes planus, the cross-sectional study performed on children noted that wearing shoes throughout early childhood can be detrimental to the development of a normal or a high medial longitudinal arch. The vulnerability for flat foot among shoe-wearing children increases if the child has an associated ligament laxity condition. The results of the study suggest that children be encouraged to play barefooted on various surfaces of terrain and that slippers and sandals are less harmful compared to closed-toe shoes. It appeared that closed-toe shoes greatly inhibited the development of the arch of the foot more so than slippers or sandals. This conclusion may be a result of the notion that intrinsic muscle activity of the arch is required to prevent slippers and sandals from falling off the child?s foot.
They make it possible for us to walk, run, and stand. With over two dozen bones, your feet are really a masterpiece of engineering. But sometimes even the best made things have flaws. One common problem is to have flatfeet, or fallen arches.
Causes
Abnormal development of the foot, producing Pes Planus, may be due to neurological problems, eg cerebral palsy, polio. Bony or ligamentous abnormalities, eg tarsal coalition (fusion of tarsal bones), accessory navicular bone. A small proportion of flexible flat feet do not correct with growth. Some of these may become rigid if the Pes Planus leads to bony changes.
Symptoms
Most patients who suffer from flat feet or fallen arches often do not complain of any symptoms whatsoever. However, on some occasions, patients may find that their feet are fatigued fairly easily and following activity on long periods of standing may have a painful foot or arch. On occasions, swelling may be seen on the inner aspect of the foot and performing certain movements may be painful and difficult. Some patients who have flat feet may find that their feet tend to roll in (over-pronate) a lot more when they walk and run. As a result, they may experience damage to the ankle joint and the Achilles tendon, as well as excessive shoe wear.
Diagnosis
If you notice that your feet are flat, but you?re not really experiencing any pain, then you?re probably okay to go without a visit to the podiatrist (unless, of course, you have a lack of feeling in your foot). You can schedule a hair appointment instead, or maybe see a movie. However, once painful symptoms start to appear, it?s better to skip the hirsute (or cinematic) experience and go see your foot doctor. Your podiatrist will likely make the diagnosis by examining your foot visually, asking about symptoms you may be experiencing, and may test your muscle strength. You may be asked to stand on your toes (in a ballerina pose, if you prefer, although that?s certainly not required), or walk around the examining room, and you may need to show the podiatrist your shoes. He or she may comment on your excellent taste in footwear, but is more likely to check your shoes for signs of wear that may indicate fallen arches. Your podiatrist may recommend X-rays, a CT scan or an MRI in order to get a look at the interior of your foot, although the best diagnosis usually comes from the doctor?s own in-person examination.
Non Surgical Treatment
Foot orthotic devices can stabilize some of the causes of flat feet, optimize muscle function and reduce the occurrence of painful symptoms. Generally, a custom-made semi-rigid functional posted orthotic is effective for flat feet. These devices are prescribed based on a thorough biomechanical examination by a qualified chiropodist/podiatrist. Over-the-counter arch supports may be helpful for mild cases, but often prove ineffective to relieve symptoms associated with flatfoot. Wear shoes with a good fit in the arch. Keep active and fit to strengthen leg and foot musculature. Control body weight to decrease load on the feet. Avoid prolonged periods weight bearing with bare feet. Taping to support strained ligaments and joints. Physical therapy modalities such as ultrasound. Referral for surgical correction a severe symptomatic flatfoot.
Surgical Treatment
Surgery for flat feet is separated into three kinds: soft tissue procedures, bone cuts, and bone fusions. Depending on the severity of the flat foot, a person?s age, and whether or not the foot is stiff determines just how the foot can be fixed. In most cases a combination of procedures are performed. With flexible flat feet, surgery is geared at maintaining the motion of the foot and recreating the arch. Commonly this may involve tendon repairs along the inside of the foot to reinforce the main tendon that lifts the arch. When the bone collapse is significant, bone procedures are included to physically rebuild the arch, and realign the heel. The presence of bunions with flat feet is often contributing to the collapse and in most situations requires correction. With rigid flat feet, surgery is focused on restoring the shape of the foot through procedures that eliminate motion. In this case, motion does not exist pre-operatively, so realigning the foot is of utmost importance. The exception, are rigid flat feet due to tarsal coalition (fused segment of bone) in the back of the foot where freeing the blockage can restore function.
Prevention
Going barefoot, particularly over terrain such as a beach where muscles are given a good workout, is good for all but the most extremely flatfooted, or those with certain related conditions such as plantar fasciitis. Ligament laxity is also among the factors known to be associated with flat feet. One medical study in India with a large sample size of children who had grown up wearing shoes and others going barefoot found that the longitudinal arches of the bare footers were generally strongest and highest as a group, and that flat feet were less common in children who had grown up wearing sandals or slippers than among those who had worn closed-toe shoes. Focusing on the influence of footwear on the prevalence of pes planus, the cross-sectional study performed on children noted that wearing shoes throughout early childhood can be detrimental to the development of a normal or a high medial longitudinal arch. The vulnerability for flat foot among shoe-wearing children increases if the child has an associated ligament laxity condition. The results of the study suggest that children be encouraged to play barefooted on various surfaces of terrain and that slippers and sandals are less harmful compared to closed-toe shoes. It appeared that closed-toe shoes greatly inhibited the development of the arch of the foot more so than slippers or sandals. This conclusion may be a result of the notion that intrinsic muscle activity of the arch is required to prevent slippers and sandals from falling off the child?s foot.