Bursitis Of The Feet Pain In Heel
Overview
In the ankle, 2 bursae are found at the level of insertion of the Achilles tendon. The superficial one is located between the skin and the tendon, and the deep one is located between the calcaneus and the tendon. The latter is the one more commonly affected by bursitis.
Causes
Bursitis has many causes, including autoimmune disorders, crystal deposition (gout and pseudogout), infectious diseases, traumatic events, and hemorrhagic disorders, as well as being secondary to overuse. Repetitive injury within the bursa results in local vasodilatation and increased vascular permeability, which stimulate the inflammatory cascade.
Symptoms
The signs and symptoms of heel bursitis can include heel pain wearing particular footwear, Pain or discomfort in the heel when walking, jogging or running, Swelling or inflammation in the heel.
Diagnosis
When you suspect you have retrocalcaneal bursitis, your foot doctor will begin by taking a complete history of the condition. A physical exam will also be performed. X-rays are usually taken on the first visit as well to determine the shape of the heel bone, joint alignment in the rearfoot, and to look for calcium deposits in the Achilles tendon. The history, exam and x-rays may sufficient for your foot surgeon to get an idea of the treatment that will be required. In some cases, it may be necessary to get an ultrasound or MRI to further evaluate the Achilles tendon or its associated bursa. While calcium deposits can show up on xray, the inflammation in the tendon and bursa will show up much better on ultrasound and MRI. The results of these tests can usually be explained on the first visit. You can then have a full understanding of how the problem started, what you can do to treat prevent it from getting worse/ You will also know which treatment will be most helpful in making your heel pain go away.
Non Surgical Treatment
You should rest from all activities that cause pain or limping. Use crutches/cane until you can walk without pain or limping. Ice. Place a plastic bag with ice on the foot for 15-20 minutes, 3-5 times a day for the first 24-72 hours. Leave the ice off at least 1 1/2 hours between applications. Compression. Lightly wrap an elastic bandage from the toes to mid calf, using even pressure. Wear this until swelling decreases. Loosen the wrap if your toes start to turn blue or feel cold. Elevate. Make sure to elevate the ankle above heart level. To improve symptoms of plantar calcaneal bursitis after the acute phasetry the baked bean tin stretch, using a baked bean tin roll the foot backwards and forwards. 2 minutes in the morning before putting the foot to the floor. 5-10 minutes every evening. Contrast foot baths. 10 minutes warm water. 10 minutes cool water morning and evening (morning may be missed if time is restricted). Stretches. Start with 10 stretches per day, holding the stretch for 30 seconds, then relax and then repeat. Continue this stretch daily until you can no longer feel it pulling on the heel, then progress to stretch. Do 10 per day holding for 30 seconds per stretch. When you can no longer feel it pulling on the heel proceed to stretches. Do 10 per day holding for 30 seconds on every stretch.
Surgical Treatment
Surgery. Though rare, particularly challenging cases of retrocalcaneal bursitis might warrant a bursectomy, in which the troublesome bursa is removed from the back of the ankle. Surgery can be effective, but operating on this boney area can cause complications, such as trouble with skin healing at the incision site. In addition to removing the bursa, a doctor may use the surgery to treat another condition associated with the retrocalcaneal bursitis. For example, a surgeon may remove a sliver of bone from the back of the heel to alter foot mechanics and reduce future friction. Any bone spurs located where the Achilles attaches to the heel may also be removed. Regardless of the conservative treatment that is provided, it is important to wait until all pain and swelling around the back of the heel is gone before resuming activities. This may take several weeks. Once symptoms are gone, a patient may make a gradual return to his or her activity level before their bursitis symptoms began. Returning to activities that cause friction or stress on the bursa before it is healed will likely cause bursitis symptoms to flare up again.
In the ankle, 2 bursae are found at the level of insertion of the Achilles tendon. The superficial one is located between the skin and the tendon, and the deep one is located between the calcaneus and the tendon. The latter is the one more commonly affected by bursitis.
Causes
Bursitis has many causes, including autoimmune disorders, crystal deposition (gout and pseudogout), infectious diseases, traumatic events, and hemorrhagic disorders, as well as being secondary to overuse. Repetitive injury within the bursa results in local vasodilatation and increased vascular permeability, which stimulate the inflammatory cascade.
Symptoms
The signs and symptoms of heel bursitis can include heel pain wearing particular footwear, Pain or discomfort in the heel when walking, jogging or running, Swelling or inflammation in the heel.
Diagnosis
When you suspect you have retrocalcaneal bursitis, your foot doctor will begin by taking a complete history of the condition. A physical exam will also be performed. X-rays are usually taken on the first visit as well to determine the shape of the heel bone, joint alignment in the rearfoot, and to look for calcium deposits in the Achilles tendon. The history, exam and x-rays may sufficient for your foot surgeon to get an idea of the treatment that will be required. In some cases, it may be necessary to get an ultrasound or MRI to further evaluate the Achilles tendon or its associated bursa. While calcium deposits can show up on xray, the inflammation in the tendon and bursa will show up much better on ultrasound and MRI. The results of these tests can usually be explained on the first visit. You can then have a full understanding of how the problem started, what you can do to treat prevent it from getting worse/ You will also know which treatment will be most helpful in making your heel pain go away.
Non Surgical Treatment
You should rest from all activities that cause pain or limping. Use crutches/cane until you can walk without pain or limping. Ice. Place a plastic bag with ice on the foot for 15-20 minutes, 3-5 times a day for the first 24-72 hours. Leave the ice off at least 1 1/2 hours between applications. Compression. Lightly wrap an elastic bandage from the toes to mid calf, using even pressure. Wear this until swelling decreases. Loosen the wrap if your toes start to turn blue or feel cold. Elevate. Make sure to elevate the ankle above heart level. To improve symptoms of plantar calcaneal bursitis after the acute phasetry the baked bean tin stretch, using a baked bean tin roll the foot backwards and forwards. 2 minutes in the morning before putting the foot to the floor. 5-10 minutes every evening. Contrast foot baths. 10 minutes warm water. 10 minutes cool water morning and evening (morning may be missed if time is restricted). Stretches. Start with 10 stretches per day, holding the stretch for 30 seconds, then relax and then repeat. Continue this stretch daily until you can no longer feel it pulling on the heel, then progress to stretch. Do 10 per day holding for 30 seconds per stretch. When you can no longer feel it pulling on the heel proceed to stretches. Do 10 per day holding for 30 seconds on every stretch.
Surgical Treatment
Surgery. Though rare, particularly challenging cases of retrocalcaneal bursitis might warrant a bursectomy, in which the troublesome bursa is removed from the back of the ankle. Surgery can be effective, but operating on this boney area can cause complications, such as trouble with skin healing at the incision site. In addition to removing the bursa, a doctor may use the surgery to treat another condition associated with the retrocalcaneal bursitis. For example, a surgeon may remove a sliver of bone from the back of the heel to alter foot mechanics and reduce future friction. Any bone spurs located where the Achilles attaches to the heel may also be removed. Regardless of the conservative treatment that is provided, it is important to wait until all pain and swelling around the back of the heel is gone before resuming activities. This may take several weeks. Once symptoms are gone, a patient may make a gradual return to his or her activity level before their bursitis symptoms began. Returning to activities that cause friction or stress on the bursa before it is healed will likely cause bursitis symptoms to flare up again.
Causes Of Hammertoe Problems
 Overview
Overview
A Hammer toes is the result of deformed toe joints, tight tendons that attach to the toe, and misaligned toe bones. The usual appearance of a hammertoe hammertoe is a toe bent upward at the middle toe joint, so that the top of this joint rubs against the top of the shoe. The remainder of the toe is bent downward so that, instead of the entire toe bearing weight, only the tip of the toe bears weight. Pain can occur on the top of the toe, the tip of the toe, or in both areas.
Causes
Ill-fitting shoes or a muscle imbalance are the most common causes of Hammer Toe. If there is an issue with a muscle in the second, third or fourth toes preventing them from straightening, Hammer Toe can result. If one of these toes is bent long enough in one position, the muscles tighten and cannot stretch out. Left untreated, surgery may be required. Women are especially prone to developing Hammer Toe because of their shoes. Hammer Toe results from shoes that don?t fit properly. Shoes that narrow toward the toe, pushing smaller toes into a bend position for extended periods of time. High heels that force the foot down into a narrow space, forcing the toes against the shoe, increasing the bend in the toe.
 Symptoms
Symptoms
People with a hammer toe will often find that a corn or callus will develop on the top of the toe, where it rubs against the top of the footwear. This can be painful when pressure is applied or when anything rubs on it. The affected joint may also be painful and appear swollen.
Diagnosis
First push up on the bottom of the metatarsal head associated with the affected toe and see if the toe straightens out. If it does, then an orthotic could correct the problem, usually with a metatarsal pad. If the toe does not straighten out when the metatarsal head is pushed up, then that indicates that contracture in the capsule and ligaments (capsule contracts because the joint was in the wrong position for too long) of the MTP joint has set in and surgery is required. Orthotics are generally required post-surgically.
Non Surgical Treatment
If you have hammer toe, avoiding tight shoes and high heels may provide relief. Initial (non-surgical) treatment for hammer toe involves wearing shoes with plenty of room in the toe area. Shoes should be at least one-half inch longer than the longest toe. Stretching and strengthening exercises for the toes (such as picking up items with the toes or stretching the toes by hand) are also recommended. Sometimes orthopedists recommend special pads, cushions, or slings to help relieve the pain of hammer toe.
Surgical Treatment
The technique the surgeon applies during the surgery depends on how much flexibility the person's affected toes still retain. If some flexibility has still been preserved in their affected toes, the hammer toes might be corrected through making a small incision into the toe so the surgeon can manipulate the tendon that is forcing the person's toes into a curved position. If, however, the person's toes have become completely rigid, the surgeon might have to do more than re-aligning the person's tendons. Some pieces of bone may have to be removed so the person's toe has the ability to straighten out. If this is the case, some pins are attached onto the person's foot afterwards to fix their bones into place while the injured tissue heals.
Do Bunions Need Surgery
Overview
 In medical terms, a bunion, or hallux valgus, is a bony bump that forms around the joint at the base of your big toe. This joint is one of the most important parts of your foot, bearing most of your body weight. The bony bump is caused by the head of the first metatarsal bone (the long bone) behind the big toe angling out from the foot. This causes the joint to swell, pushing the big toe in towards the adjacent toes. The result is pain on the side of your foot, arch pain, and discomfort throughout the adjacent toes as well.
In medical terms, a bunion, or hallux valgus, is a bony bump that forms around the joint at the base of your big toe. This joint is one of the most important parts of your foot, bearing most of your body weight. The bony bump is caused by the head of the first metatarsal bone (the long bone) behind the big toe angling out from the foot. This causes the joint to swell, pushing the big toe in towards the adjacent toes. The result is pain on the side of your foot, arch pain, and discomfort throughout the adjacent toes as well.
Causes
There is some debate about the main cause of foot bunion pain, but they tend to fall into 2 categories. Genetics. There is a definite genetic link, meaning that if someone in your family suffers from a hallux abducto valgus, there is a high chance that you will too, although this is not always the case. It may be due to an abnormal foot position such as flat feet, or a medical condition such as hypermobility (where your joints are overly flexible) or arthritis (e.g. rheumatoid arthritis or gout). Regularly wearing high heels with a pointed toe puts you at high risk for developing foot bunions. Ill-Fitting Footwear. Poorly fitting shoes are thought to be the other common cause of foot bunion pain. Frequent wear of tight fitting shoes or high heels places excessive pressure on the big toe pushing it into the classic hallux abducto valgus position.
Symptoms
Symptoms, which occur at the site of the bunion, may include pain or soreness, inflammation and redness, a burning sensation, possible numbness. Symptoms occur most often when wearing shoes that crowd the toes, such as shoes with a tight toe box or high heels. This may explain why women are more likely to have symptoms than men. In addition, spending long periods of time on your feet can aggravate the symptoms of bunions.
Diagnosis
Bunions are readily apparent, you can see the prominence at the base of the big toe or side of the foot. However, to fully evaluate your condition, the Podiatrist may arrange for x-rays to be taken to determine the degree of the deformity and assess the changes that have occurred. Because bunions are progressive, they don't go away, and will usually get worse over time. But not all cases are alike, some bunions progress more rapidly than others. There is no clear-cut way to predict how fast a bunion will get worse. The severity of the bunion and the symptoms you have will help determine what treatment is recommended for you.
Non Surgical Treatment
Apply special pads and dressings to protect the bunion from shoe pressure. Inject steroid and local anesthetic around the bunion to reduce inflammation. This is especially useful if there is an associated bursitis. Recommend commercially available or custom made shoes. Prescribe functional orthotics to correct faulty foot function, and help prevent worsening of the deformity. Recommend bunion surgery to correct the deformity. 
Surgical Treatment
Bunion surgery can be performed under local or general anaesthetic. The operation usually takes between half an hour to an hour. There are several types of bunionectomies. Some involve removal and realignment of the bones in your foot. Mild bunion problems can sometimes be resolved using soft tissue release or tightening. For some very severe cases bones of the big toe are fused or the bunion is cut out along with some of the bone at the base of the toe. Be sure and discuss which type of operation you will have with your surgeon. With any type of bunionectomy your surgeon will make one or more incisions (cuts) near your big toe. They will use instruments to trim the bones and remove the bunion. Wire, screws or plates may also be used to hold the new joint in place.
The Treatment And Cause Of Over-Pronation Of The Foot
Overview
Pronation is a normal motion that our feet make as they walk. With each step, the heel touches the ground first, then the foot rolls forward to the toes, causing the ankle to roll inward slightly and the arch to flatten out. That?s normal. But when that rolling inward becomes more pronounced, that?s over-pronation, which is a big problem. You can usually see over-pronation by looking at the back of the leg and foot. The Achilles tendon normally runs straight down from the leg to the foot, hitting the floor at a perpendicular angle. In feet that over-pronate, the Achilles tendon will be at a slight angle to the ground and the ankle bone will appear more prominent than usual.
Causes
Unless there is a severe, acute injury, overpronation develops as a gradual biomechanical distortion. Several factors contribute to developing overpronation, including tibialis posterior weakness, ligament weakness, excess weight, pes planus (flat foot), genu valgum (knock knees), subtalar eversion, or other biomechanical distortions in the foot or ankle. Tibialis posterior weakness is one of the primary factors leading to overpronation. Pronation primarily is controlled by the architecture of the foot and eccentric activation of the tibialis posterior. If the tibialis posterior is weak, the muscle cannot adequately slow the natural pronation cycle.
Symptoms
Due to the laxity of the soft tissue structures of the foot, and the fact that the joints are not held together properly, the bones of the feet shift. When this occurs, the muscles that attach to these bones must also shift, or twist, in order to attach to these bones. The strongest and most important muscles that attach to our foot bones come from our lower leg. So, as these muscles course down the leg and across the ankle, they must twist to maintain their proper attachments in the foot. This twisting of these muscles will cause shin splints, Achilles Tendonitis, generalized tendonitis, fatigue, muscle aches and pains, cramps, ankle sprains, and loss of muscular efficiency (reducing walking and running speed and endurance). The problems we see in the feet, which are due to over-pronation include bunions, heel spurs, plantar fasciitis, fallen and painful arches, hammertoes, metatarsalgia (ball of foot pain), and calluses.
Diagnosis
The best way to discover whether you have a normal gait, or if you overpronate, is to visit a specialty run shop, an exercise physiologist, a podiatrist or a physical therapist who specializes in working with athletes. A professional can analyze your gait, by watching you either walk or run, preferably on a treadmill. Some facilities can videotape your gait, then analyze the movement of your feet in slow-motion. Another (and less costly) way is to look at the bottom of an older pair of run shoes. Check the wear pattern. A person with a normal gait will generally see wear evenly across the heel and front of the shoe. A person who overpronates will likely see more wear on the OUTside of the heel and more wear on the INside of the forefoot (at the ball). A person who supinates will see wear all along the outer edges of the shoe. You can also learn about your gait by looking at your arches. Look at the shape your wet feet leave on a piece of paper or a flat walking surface.
Non Surgical Treatment
Studies have shown that the most effective way to dexrease a high Q angle and lower the biomechanical stresses on the knee joint is to prevent excessive pronation with custom-maflexible orthotics. One study found that using soft corrective orthotics was more effective in reduknee pain than a traditional exercise program. A more recent study showed that Q angle asymmetries, secondary to excessive pronation affecting knee alignment, can be effectivecontrolled or corrected utilizing custom-made, flexible orthotics. Another project involving meof a running club determined that 75% of those using orthotics eliminated or greatly reduced pain in the feet, ankles, shins, knees and hips
Prevention
Massage and stretch the calves to increase dorsiflexion at the foot/ankle. Dorsiflexion is the bending at the ankle. By improving the dorsiflexion, one will have more flexibility at the ankle, which will allow the foot to over-pronate less. Massage the IT Band with a foam roller or tennis ball to quiet down the tightness throughout this part of the leg. The IT Band attaches from the glute maximus and runs down the side of the leg into the knee area. When the IT Band is tight it will accelerate the force of the leg moving inward, which will cause the foot to move inward as well. It is often that tightness through the IT Band that promotes over-pronation. Decreasing over-pronation, which is very prominent in runners, will help add endurance, speed and efficiency to your run and ultimately place less stress on your body.
Pronation is a normal motion that our feet make as they walk. With each step, the heel touches the ground first, then the foot rolls forward to the toes, causing the ankle to roll inward slightly and the arch to flatten out. That?s normal. But when that rolling inward becomes more pronounced, that?s over-pronation, which is a big problem. You can usually see over-pronation by looking at the back of the leg and foot. The Achilles tendon normally runs straight down from the leg to the foot, hitting the floor at a perpendicular angle. In feet that over-pronate, the Achilles tendon will be at a slight angle to the ground and the ankle bone will appear more prominent than usual.
Causes
Unless there is a severe, acute injury, overpronation develops as a gradual biomechanical distortion. Several factors contribute to developing overpronation, including tibialis posterior weakness, ligament weakness, excess weight, pes planus (flat foot), genu valgum (knock knees), subtalar eversion, or other biomechanical distortions in the foot or ankle. Tibialis posterior weakness is one of the primary factors leading to overpronation. Pronation primarily is controlled by the architecture of the foot and eccentric activation of the tibialis posterior. If the tibialis posterior is weak, the muscle cannot adequately slow the natural pronation cycle.
Symptoms
Due to the laxity of the soft tissue structures of the foot, and the fact that the joints are not held together properly, the bones of the feet shift. When this occurs, the muscles that attach to these bones must also shift, or twist, in order to attach to these bones. The strongest and most important muscles that attach to our foot bones come from our lower leg. So, as these muscles course down the leg and across the ankle, they must twist to maintain their proper attachments in the foot. This twisting of these muscles will cause shin splints, Achilles Tendonitis, generalized tendonitis, fatigue, muscle aches and pains, cramps, ankle sprains, and loss of muscular efficiency (reducing walking and running speed and endurance). The problems we see in the feet, which are due to over-pronation include bunions, heel spurs, plantar fasciitis, fallen and painful arches, hammertoes, metatarsalgia (ball of foot pain), and calluses.
Diagnosis
The best way to discover whether you have a normal gait, or if you overpronate, is to visit a specialty run shop, an exercise physiologist, a podiatrist or a physical therapist who specializes in working with athletes. A professional can analyze your gait, by watching you either walk or run, preferably on a treadmill. Some facilities can videotape your gait, then analyze the movement of your feet in slow-motion. Another (and less costly) way is to look at the bottom of an older pair of run shoes. Check the wear pattern. A person with a normal gait will generally see wear evenly across the heel and front of the shoe. A person who overpronates will likely see more wear on the OUTside of the heel and more wear on the INside of the forefoot (at the ball). A person who supinates will see wear all along the outer edges of the shoe. You can also learn about your gait by looking at your arches. Look at the shape your wet feet leave on a piece of paper or a flat walking surface.
Non Surgical Treatment
Studies have shown that the most effective way to dexrease a high Q angle and lower the biomechanical stresses on the knee joint is to prevent excessive pronation with custom-maflexible orthotics. One study found that using soft corrective orthotics was more effective in reduknee pain than a traditional exercise program. A more recent study showed that Q angle asymmetries, secondary to excessive pronation affecting knee alignment, can be effectivecontrolled or corrected utilizing custom-made, flexible orthotics. Another project involving meof a running club determined that 75% of those using orthotics eliminated or greatly reduced pain in the feet, ankles, shins, knees and hips
Prevention
Massage and stretch the calves to increase dorsiflexion at the foot/ankle. Dorsiflexion is the bending at the ankle. By improving the dorsiflexion, one will have more flexibility at the ankle, which will allow the foot to over-pronate less. Massage the IT Band with a foam roller or tennis ball to quiet down the tightness throughout this part of the leg. The IT Band attaches from the glute maximus and runs down the side of the leg into the knee area. When the IT Band is tight it will accelerate the force of the leg moving inward, which will cause the foot to move inward as well. It is often that tightness through the IT Band that promotes over-pronation. Decreasing over-pronation, which is very prominent in runners, will help add endurance, speed and efficiency to your run and ultimately place less stress on your body.
Severs Disease Physiotherapy
Overview
Sever's Disease, also known as calcaneal apophysitis, is a disease of the growth plate of the bone and is characterized by pain in the heel of a child's foot, typically brought on by some form of injury or trauma. This condition is most common in children ages 10 to 15 and is frequently seen in active soccer, football, or baseball players. Sport shoes with cleats are also known to aggravate the condition. The disease mimics Achilles tendonitis, an inflammation of the tendon attached to the back of the heel. A tight Achilles tendon contributes to Sever's Disease by pulling excessively on the growth plate of the heel bone (calcaneus). Treatment includes cutting back on sports activities, calf muscle stretching exercises, heel cushions in the shoes, icing, and/or anti-inflammatory medications. Note: Please consult your physician before taking any medications.
Causes
Apart from age, other factors that may contribute to developing Sever?s disease include physical activity, any form of exercise that is weight bearing through the legs or stresses the soft tissue can exacerbate the pain of the disease, External factors, for example, running on hard surfaces or wearing inappropriate shoes during sport Overuse injury, very active children may repeatedly but subtly injure the bones, muscles and tendons of their feet and ankles. In time, the accumulated injuries cause symptoms.
Symptoms
The most common symptom of Sever's disease is acute pain felt in the heel when a child engages in physical activity such as walking, jumping or running. Children who are very active athletes are among the group most susceptible to experiencing Sever's disease because of the extreme stress and tension they place on their growing feet. Improper pronation, the rolling movement of the foot during walking or running, and obesity are all additional conditions linked to causing Sever's disease.
Diagnosis
A doctor can usually tell that a child has Sever's disease based on the symptoms reported. To confirm the diagnosis, the doctor will probably examine the heels and ask about the child's activity level and participation in sports. The doctor might also use the squeeze test, squeezing the back part of the heel from both sides at the same time to see if doing so causes pain. The doctor might also ask the child to stand on tiptoes to see if that position causes pain. Although imaging tests such as X-rays generally are not that helpful in diagnosing Sever's disease, some doctors order them to rule out other problems, such as fractures. Sever's disease cannot be seen on an X-ray.
Non Surgical Treatment
Most patients with Sever?s Disease can be treated with a self-guided home exercise program. Your healthcare provider will discuss with you if a prescription for formal physical therapy is indicated instead of a self-directed home or school exercise program. Rest (protection of the heel). Ice (Ice 20 minutes at a time, 2-3 times a day). Gel heel pads / inserts. Anti-inflammatory medication. Well cushioned pair of shoes. Brace (Cheetah) *Generally given for those who cannot wear shoes during their sport. Low impact aerobic training such as walking, riding a bike, elliptical or swimming. Home exercise program focusing on increasing the flexibility of the heel cord and calf muscle.
Recovery
Severs disease is a self limiting condition that gradually resolves as the patient moves towards skeletal maturity. This usually takes between 6 to 12 months, but may persist for as long as 2 years. With appropriate management, symptoms may resolve in a number of weeks. Patients with Severs disease typically improve gradually over time and full function is restored.
Sever's Disease, also known as calcaneal apophysitis, is a disease of the growth plate of the bone and is characterized by pain in the heel of a child's foot, typically brought on by some form of injury or trauma. This condition is most common in children ages 10 to 15 and is frequently seen in active soccer, football, or baseball players. Sport shoes with cleats are also known to aggravate the condition. The disease mimics Achilles tendonitis, an inflammation of the tendon attached to the back of the heel. A tight Achilles tendon contributes to Sever's Disease by pulling excessively on the growth plate of the heel bone (calcaneus). Treatment includes cutting back on sports activities, calf muscle stretching exercises, heel cushions in the shoes, icing, and/or anti-inflammatory medications. Note: Please consult your physician before taking any medications.
Causes
Apart from age, other factors that may contribute to developing Sever?s disease include physical activity, any form of exercise that is weight bearing through the legs or stresses the soft tissue can exacerbate the pain of the disease, External factors, for example, running on hard surfaces or wearing inappropriate shoes during sport Overuse injury, very active children may repeatedly but subtly injure the bones, muscles and tendons of their feet and ankles. In time, the accumulated injuries cause symptoms.
Symptoms
The most common symptom of Sever's disease is acute pain felt in the heel when a child engages in physical activity such as walking, jumping or running. Children who are very active athletes are among the group most susceptible to experiencing Sever's disease because of the extreme stress and tension they place on their growing feet. Improper pronation, the rolling movement of the foot during walking or running, and obesity are all additional conditions linked to causing Sever's disease.
Diagnosis
A doctor can usually tell that a child has Sever's disease based on the symptoms reported. To confirm the diagnosis, the doctor will probably examine the heels and ask about the child's activity level and participation in sports. The doctor might also use the squeeze test, squeezing the back part of the heel from both sides at the same time to see if doing so causes pain. The doctor might also ask the child to stand on tiptoes to see if that position causes pain. Although imaging tests such as X-rays generally are not that helpful in diagnosing Sever's disease, some doctors order them to rule out other problems, such as fractures. Sever's disease cannot be seen on an X-ray.
Non Surgical Treatment
Most patients with Sever?s Disease can be treated with a self-guided home exercise program. Your healthcare provider will discuss with you if a prescription for formal physical therapy is indicated instead of a self-directed home or school exercise program. Rest (protection of the heel). Ice (Ice 20 minutes at a time, 2-3 times a day). Gel heel pads / inserts. Anti-inflammatory medication. Well cushioned pair of shoes. Brace (Cheetah) *Generally given for those who cannot wear shoes during their sport. Low impact aerobic training such as walking, riding a bike, elliptical or swimming. Home exercise program focusing on increasing the flexibility of the heel cord and calf muscle.
Recovery
Severs disease is a self limiting condition that gradually resolves as the patient moves towards skeletal maturity. This usually takes between 6 to 12 months, but may persist for as long as 2 years. With appropriate management, symptoms may resolve in a number of weeks. Patients with Severs disease typically improve gradually over time and full function is restored.
The Causes Of Posterior Tibial Tendon Dysfunction (PTTD) ?
Overview
Adult Acquired Flatfoot (Posterior Tibial Tendon Dysfunction) is a painful, progressive deformity in adults. It results from a gradual stretch (attenuation) of the tibialis posterior tendon and the ligaments that support your foot?s arch. This stretching causes the tendon to lose strength and function. Many people have flat feet and do not experience pain. However, pain occurs with Adult Acquired Flatfoot because the tendons and ligaments have been torn. Once the vital ligaments and posterior tibial tendon are lost, there is no longer anything holding the arch of the foot in place. 
Causes
Women are affected by Adult Acquired Flatfoot four times more frequently than men. Adult Flatfoot generally occurs in middle to older age people. Most people who acquire the condition already have flat feet. One arch begins to flatten more, then pain and swelling develop on the inside of the ankle. This condition generally affects only one foot. It is unclear why women are affected more often than men. But factors that may increase your risk of Adult Flatfoot include diabetes, hypertension, and obesity.
Symptoms
Depending on the cause of the flatfoot, a patient may experience one or more of the different symptoms here. Pain along the course of the posterior tibial tendon which lies on the inside of the foot and ankle. This can be associated with swelling on the inside of the ankle. Pain that is worse with activity. High intensity or impact activities, such as running, can be very difficult. Some patients can have difficulty walking or even standing for long periods of time. When the foot collapses, the heel bone may shift position and put pressure on the outside ankle bone (fibula). This can cause pain on the outside of the ankle. Arthritis in the heel also causes this same type of pain. Patients with an old injury or arthritis in the middle of the foot can have painful, bony bumps on the top and inside of the foot. These make shoewear very difficult. Occasionally, the bony spurs are so large that they pinch the nerves which can result in numbness and tingling on the top of the foot and into the toes. Diabetics may only notice swelling or a large bump on the bottom of the foot. Because their sensation is affected, people with diabetes may not have any pain. The large bump can cause skin problems and an ulcer (a sore that does not heal) may develop if proper diabetic shoewear is not used.
Diagnosis
Posterior Tibial Tendon Dysfunction is diagnosed with careful clinical observation of the patient?s gait (walking), range of motion testing for the foot and ankle joints, and diagnostic imaging. People with flatfoot deformity walk with the heel angled outward, also called over-pronation. Although it is normal for the arch to impact the ground for shock absorption, people with PTTD have an arch that fully collapses to the ground and does not reform an arch during the entire gait period. After evaluating the ambulation pattern, the foot and ankle range of motion should be tested. Usually the affected foot will have decreased motion to the ankle joint and the hindfoot. Muscle strength may also be weaker as well. An easy test to perform for PTTD is the single heel raise where the patient is asked to raise up on the ball of his or her effected foot. A normal foot type can lift up on the toes without pain and the heel will invert slightly once the person has fully raised the heel up during the test. In early phases of PTTD the patient may be able to lift up the heel but the heel will not invert. An elongated or torn posterior tibial tendon, which is a mid to late finding of PTTD, will prohibit the patient from fully rising up on the heel and will cause intense pain to the arch. Finally diagnostic imaging, although used alone cannot diagnose PTTD, can provide additional information for an accurate diagnosis of flatfoot deformity. Xrays of the foot can show the practitioner important angular relationships of the hindfoot and forefoot which help diagnose flatfoot deformity. Most of the time, an MRI is not needed to diagnose PTTD but is a tool that should be considered in advanced cases of flatfoot deformity. If a partial tear of the posterior tibial tendon is of concern, then an MRI can show the anatomic location of the tear and the extensiveness of the injury.
Non surgical Treatment
Nonoperative therapy for adult-acquired flatfoot is a reasonable treatment option that is likely to be beneficial for most patients. In this article, we describe the results of a retrospective cohort study that focused on nonoperative measures, including bracing, physical therapy, and anti-inflammatory medications, used to treat adult-acquired flatfoot in 64 consecutive patients. The results revealed the incidence of successful nonsurgical treatment to be 87.5% (56 of 64 patients), over the 27-month observation period. Overall, 78.12% of the patients with adult-acquired flatfoot were obese (body mass index [BMI] = 30), and 62.5% of the patients who failed nonsurgical therapy were obese; however, logistic regression failed to show that BMI was statistically significantly associated with the outcome of treatment. The use of any form of bracing was statistically significantly associated with successful nonsurgical treatment (fully adjusted OR = 19.8621, 95% CI 1.8774 to 210.134), whereas the presence of a split-tear of the tibialis posterior on magnetic resonance image scans was statistically significantly associated with failed nonsurgical treatment (fully adjusted OR = 0.016, 95% CI 0.0011 to 0.2347). The results of this investigation indicate that a systematic nonsurgical treatment approach to the treatment of the adult-acquired flatfoot deformity can be successful in most cases. 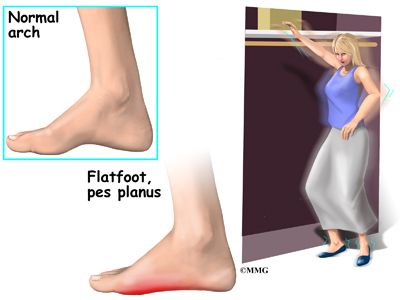
Surgical Treatment
Stage two deformities are less responsive to conservative therapies that can be effective in mild deformities. Bone procedures are necessary at this stage in order to recreate the arch and stabilize the foot. These procedures include isolated fusion procedures, bone grafts, and/or the repositioning of bones through cuts called osteotomies. The realigned bones are generally held in place with screws, pins, plates, or staples while the bone heals. A tendon transfer may or may not be utilized depending on the condition of the posterior tibial tendon. Stage three deformities are better treated with surgical correction, in healthy patients. Patients that are unable to tolerate surgery or the prolonged healing period are better served with either arch supports known as orthotics or bracing such as the Richie Brace. Surgical correction at this stage usually requires fusion procedures such as a triple or double arthrodesis. This involves fusing the two or three major bones in the back of the foot together with screws or pins. The most common joints fused together are the subtalar joint, talonavicular joint, and the calcaneocuboid joint. By fusing the bones together the surgeon is able to correct structural deformity and alleviate arthritic pain. Tendon transfer procedures are usually not beneficial at this stage. Stage four deformities are treated similarly but with the addition of fusing the ankle joint.
Pain In The Arch Causes Symptoms And Treatments
Overview
One of those often-painful soft tissue that attaches to heel spurs at the bottom of the foot is called "plantar fascia". Fascia, located throughout the body, is a fibrous connective tissue similar to a ligament. You can see fascia when you handle meat. It is the white, connective tissue separating layers of meat or attaching to bones. The "plantar" fascia in our bodies is that fascia which is seen on the bottom (or plantar portion) of the foot, extending from the heel bone to the ball of the foot. Compared to other fascia around the body, plantar fascia is very thick and very strong. It has to be strong because of the tremendous amount of force it must endure when you walk, run or jump. But while the plantar fascia is a strong structure, it can still get injured, most commonly when it is stretched beyond its normal length over long periods of time. When plantar fascia is injured, the condition is called "plantar fasciitis", which is usualy pronounced either "plan-tar fash-I-tis" or "plan-tar-fash-ee-I-tis." (Adding "-itis" to the end of a word means that structure is inflamed.) It is sometimes known more simply as 'fasciitis'. Plantar fasciitis is the most common type of arch pain.

Causes
The plantar fascia is designed to absorb the high stresses and strains we place on our feet. But, sometimes, too much pressure damages or tears the tissues. The body's natural response to injury is inflammation, which results in the heel pain and stiffness of plantar fasciitis.
Symptoms
The primary symptom is pain or aching in the arch area. This can be accompanied by inflammation and tenderness. If the pain is caused by the plantar fascia, it is likely to be considerably more severe in the mornings due to the muscles being unused.
Diagnosis
Your doctor may order imaging tests to help make sure your heel pain is caused by plantar fasciitis and not another problem. X-rays provide clear images of bones. They are useful in ruling out other causes of heel pain, such as fractures or arthritis. Heel spurs can be seen on an x-ray. Other imaging tests, such as magnetic resonance imaging (MRI) and ultrasound, are not routinely used to diagnose plantar fasciitis. They are rarely ordered. An MRI scan may be used if the heel pain is not relieved by initial treatment methods.
Non Surgical Treatment
Treatment for a high arch foot or Charcot Marie Tooth disorder depends on the extent of deformity and the amount of disability experienced by the patient. Depending upon the symptoms, treatment may include. Changing the shoes. Special orthotic supports (devices that support, adjust, or accommodate the foot deformity). Cushioning pads. Foot and ankle braces or surgery.

Surgical Treatment
In cases where cast immobilization, orthoses and shoe therapy have failed, surgery is the next alternative. The goal of surgery and non-surgical treatment is to eliminate pain, stop progression of the deformity and improve mobility of the patient. Opinions vary as to the best surgical treatment for adult acquired flatfoot. Procedures commonly used to correct the condition include tendon debridement, tendon transfers, osteotomies (cutting and repositioning of bone) and joint fusions.
Prevention
To prevent arch pain, it is important to build up slowly to your exercise routine while wearing arch supports inside training shoes. By undertaking these simple measures you can prevent the discomfort of arch pain which can otherwise linger for many months. While you allow the foot to recover, it will help to undertake low impact exercises (such as swimming or water aerobics).
Stretching Exercises
Inchworm. Stand with your weight on one foot. Raise the metatarsal heads of the unweighted foot while you pull its heel closer to your toes. Next, raise your toes toward the ceiling, and then relax your whole foot with it flat on the floor. Your foot should move like an inchworm across the floor. Reps 6-7 for each foot. Horsepawing. Stand with your weight on one foot and the other foot slightly in front of you. Raise the metatarsal heads on the front foot. Lift your heel ever so slightly off the ground, maintaining the raised metatarsal heads, and pull your foot toward you so that it ends up behind you. Return this foot to the starting position in front of you. You should really feel this one in your arch. Reps. 6-7 for each foot. Toe pushups. Sit in a chair with your feet resting on the floor. Raise your heel as high as you can while keeping your toes flat on the floor. This is the starting position. Using your toe muscles, roll your foot upward until the weight of your foot is resting on the ends of your toes, like a dancer standing on point in toe shoes. Roll back down to the starting position. Reps. 10-20 for each foot. Sand scraping. Pretend you are at the beach standing in loose sand. Use your big toe to pull sand inward toward your body, with your little toe off the ground. Then use your little toe to push it away, with your big toe off the ground. Reps. 10 for each foot. Now reverse the exercise: pull the sand inward with your little toe and push it away with your big toe. Reps. 10 for each foot.
One of those often-painful soft tissue that attaches to heel spurs at the bottom of the foot is called "plantar fascia". Fascia, located throughout the body, is a fibrous connective tissue similar to a ligament. You can see fascia when you handle meat. It is the white, connective tissue separating layers of meat or attaching to bones. The "plantar" fascia in our bodies is that fascia which is seen on the bottom (or plantar portion) of the foot, extending from the heel bone to the ball of the foot. Compared to other fascia around the body, plantar fascia is very thick and very strong. It has to be strong because of the tremendous amount of force it must endure when you walk, run or jump. But while the plantar fascia is a strong structure, it can still get injured, most commonly when it is stretched beyond its normal length over long periods of time. When plantar fascia is injured, the condition is called "plantar fasciitis", which is usualy pronounced either "plan-tar fash-I-tis" or "plan-tar-fash-ee-I-tis." (Adding "-itis" to the end of a word means that structure is inflamed.) It is sometimes known more simply as 'fasciitis'. Plantar fasciitis is the most common type of arch pain.
Causes
The plantar fascia is designed to absorb the high stresses and strains we place on our feet. But, sometimes, too much pressure damages or tears the tissues. The body's natural response to injury is inflammation, which results in the heel pain and stiffness of plantar fasciitis.
Symptoms
The primary symptom is pain or aching in the arch area. This can be accompanied by inflammation and tenderness. If the pain is caused by the plantar fascia, it is likely to be considerably more severe in the mornings due to the muscles being unused.
Diagnosis
Your doctor may order imaging tests to help make sure your heel pain is caused by plantar fasciitis and not another problem. X-rays provide clear images of bones. They are useful in ruling out other causes of heel pain, such as fractures or arthritis. Heel spurs can be seen on an x-ray. Other imaging tests, such as magnetic resonance imaging (MRI) and ultrasound, are not routinely used to diagnose plantar fasciitis. They are rarely ordered. An MRI scan may be used if the heel pain is not relieved by initial treatment methods.
Non Surgical Treatment
Treatment for a high arch foot or Charcot Marie Tooth disorder depends on the extent of deformity and the amount of disability experienced by the patient. Depending upon the symptoms, treatment may include. Changing the shoes. Special orthotic supports (devices that support, adjust, or accommodate the foot deformity). Cushioning pads. Foot and ankle braces or surgery.
Surgical Treatment
In cases where cast immobilization, orthoses and shoe therapy have failed, surgery is the next alternative. The goal of surgery and non-surgical treatment is to eliminate pain, stop progression of the deformity and improve mobility of the patient. Opinions vary as to the best surgical treatment for adult acquired flatfoot. Procedures commonly used to correct the condition include tendon debridement, tendon transfers, osteotomies (cutting and repositioning of bone) and joint fusions.
Prevention
To prevent arch pain, it is important to build up slowly to your exercise routine while wearing arch supports inside training shoes. By undertaking these simple measures you can prevent the discomfort of arch pain which can otherwise linger for many months. While you allow the foot to recover, it will help to undertake low impact exercises (such as swimming or water aerobics).
Stretching Exercises
Inchworm. Stand with your weight on one foot. Raise the metatarsal heads of the unweighted foot while you pull its heel closer to your toes. Next, raise your toes toward the ceiling, and then relax your whole foot with it flat on the floor. Your foot should move like an inchworm across the floor. Reps 6-7 for each foot. Horsepawing. Stand with your weight on one foot and the other foot slightly in front of you. Raise the metatarsal heads on the front foot. Lift your heel ever so slightly off the ground, maintaining the raised metatarsal heads, and pull your foot toward you so that it ends up behind you. Return this foot to the starting position in front of you. You should really feel this one in your arch. Reps. 6-7 for each foot. Toe pushups. Sit in a chair with your feet resting on the floor. Raise your heel as high as you can while keeping your toes flat on the floor. This is the starting position. Using your toe muscles, roll your foot upward until the weight of your foot is resting on the ends of your toes, like a dancer standing on point in toe shoes. Roll back down to the starting position. Reps. 10-20 for each foot. Sand scraping. Pretend you are at the beach standing in loose sand. Use your big toe to pull sand inward toward your body, with your little toe off the ground. Then use your little toe to push it away, with your big toe off the ground. Reps. 10 for each foot. Now reverse the exercise: pull the sand inward with your little toe and push it away with your big toe. Reps. 10 for each foot.